- The Step 1 Newsletter
- Posts
- ☕️ Which of the following medications is the most likely cause of this patient's condition?
☕️ Which of the following medications is the most likely cause of this patient's condition?
Morning Quiz 126 ☕️
Dr. Shoaib Ahmad Baig
June 15, 2025
Morning Quiz ☕️
A 68-year-old woman is brought to the emergency department due to worsening lethargy.
History of Present Illness
Family reports:
Headache and nausea for the past several days.
Today, she became confused and lethargic.
Medical history:
Seizure disorder
Hypertension
Type 2 diabetes mellitus
Bipolar disorder
Current medications: Multiple (unspecified).
Physical Examination
Vital signs: Within normal limits.
General: Somnolent, responds only to painful stimuli.
Cardiovascular:
JVP normal, heart sounds normal.
Respiratory: Lungs clear to auscultation.
Extremities: No edema.
Mucous membranes: Moist.
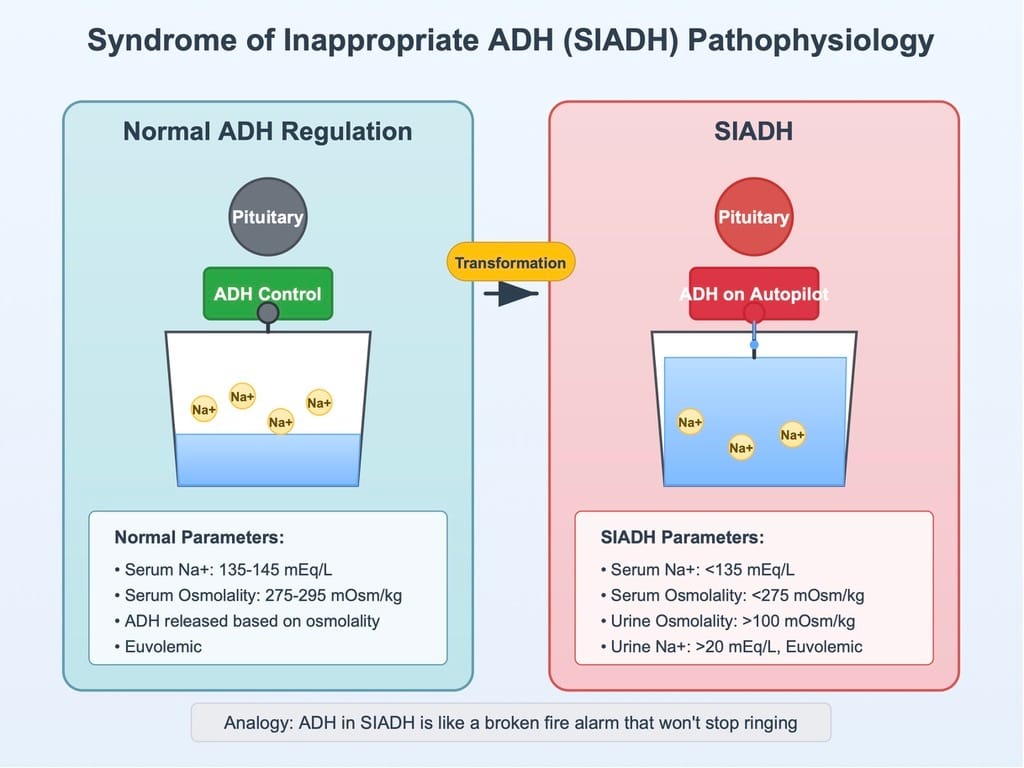
Laboratory Findings
Serum sodium: 118 mEq/L (normal: 135–145).
Renal function: BUN and creatinine within normal limits.
Osmolality:
Serum osmolality: Low
Urine osmolality: High
Question
Which of the following medications is the most likely cause of this patient's condition?
Options:
A. Canagliflozin
B. Carbamazepine
C. Furosemide
D. Lithium
E. Spironolactone
Correct Answer 🎯: B. Carbamazepine
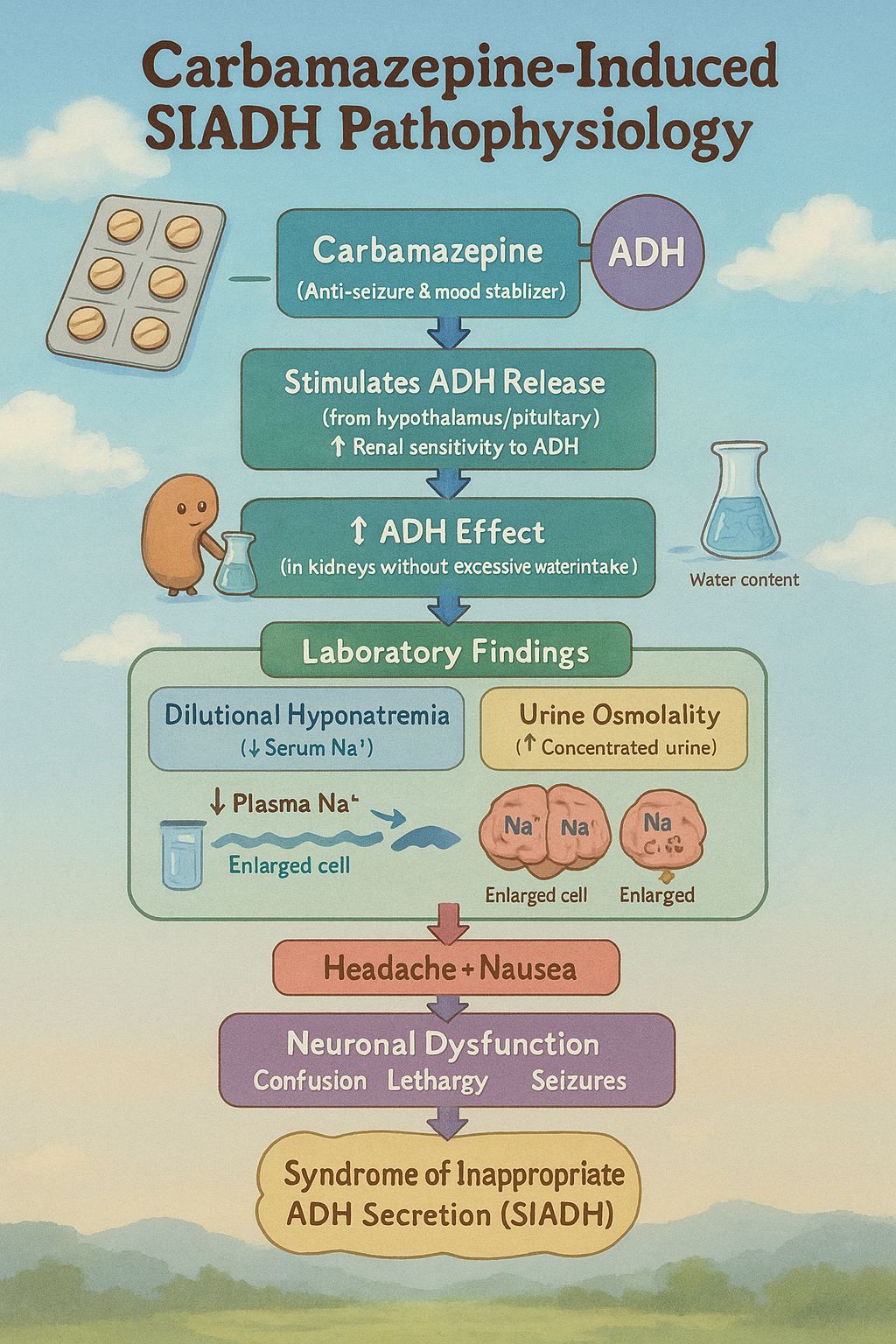
⚙️
Carbamazepine (Anti-seizure & mood stabilizer)
⬇
Stimulates ADH release (from hypothalamus/pituitary )
or ↑ Renal sensitivity to ADH
⬇
↑ ADH effect despite normal serum osmolality
⬇
↑ water reabsorption in kidneys without appropriate osmotic trigger
⬇
Dilutional hyponatremia (Serum Na⁺ 118 mEq/L, ↓ serum osmolality)
⬇
↑ Urine osmolality (Kidneys still concentrating urine due to ADH action)
⬇
↓ Plasma Na⁺ → Water shifts into brain cells (↑ ICF)
⬇
(Brain cells swell )
⬇
Cerebral edema
⬇
Headache + Nausea
(due to cerebral edema → ↑ intracranial pressure)
⬇
Neuronal dysfunction
⬇
Confusion → Lethargy → Somnolence (responds to pain only)
🧠 Syndrome of Inappropriate ADH Secretion (SIADH)
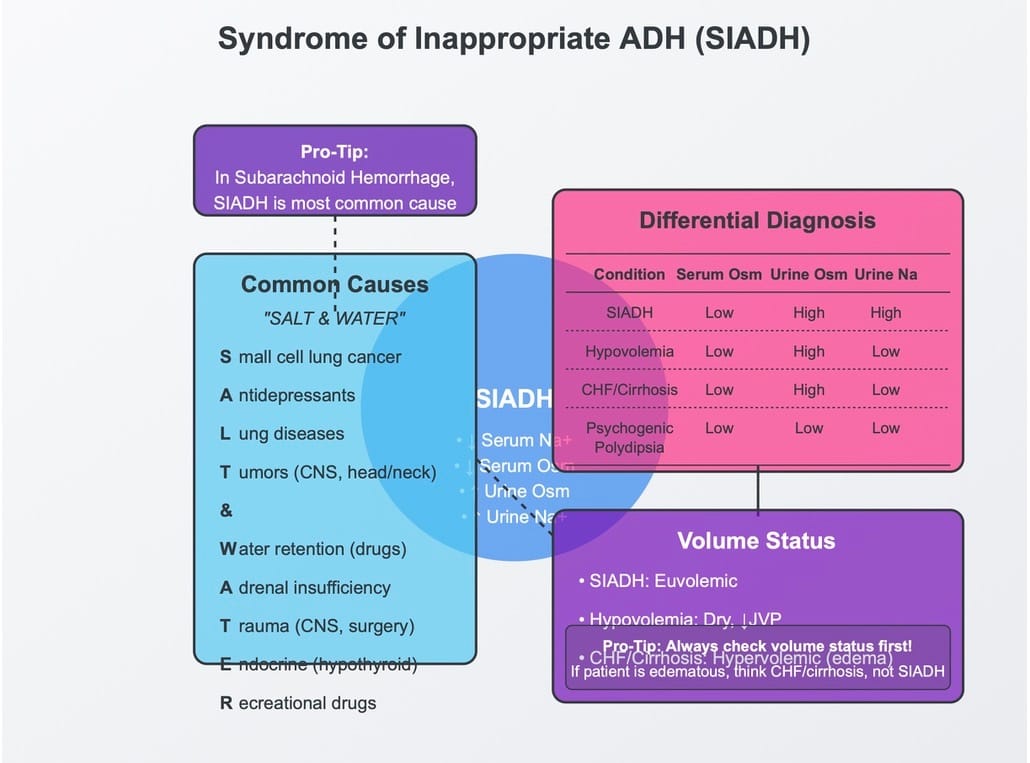
Differential Table ⚖️
Differential ⚖️ | Mechanism ⚙️ | Why Incorrect? 🔴 |
|---|---|---|
Canagliflozin(SGLT2 inhibitor) | Blocks glucose reabsorption in PCT → ↑ Glucose in tubule → Osmotic diuresis → ↑ Water loss | Causes hypovolemia + hypernatremia(opposite of this case) |
Furosemide(Loop diuretic) | Inhibits Na⁺/K⁺/2Cl⁻ pump in TAL → ↓ Na⁺ reabsorption → ↓ Medullary gradient → ↓ Water reabsorption | Causes ↓ urine osmolality, hypovolemia(Not matching: urine is concentrated + euvolemic) |
Lithium | Damages principal cells → Blocks ADH action → Nephrogenic DI → ↑ Water loss → ↑ Serum Na⁺ | Hypernatremia + dilute urine expected (opposite of findings) |
Spironolactone | Aldosterone antagonist → ↑ Na⁺ excretion, ↑ K⁺ retention → Mild volume loss | Would cause dry mucosa, ↓ JVP, ↓ BP → Not observed (mucosa moist, JVP normal) |
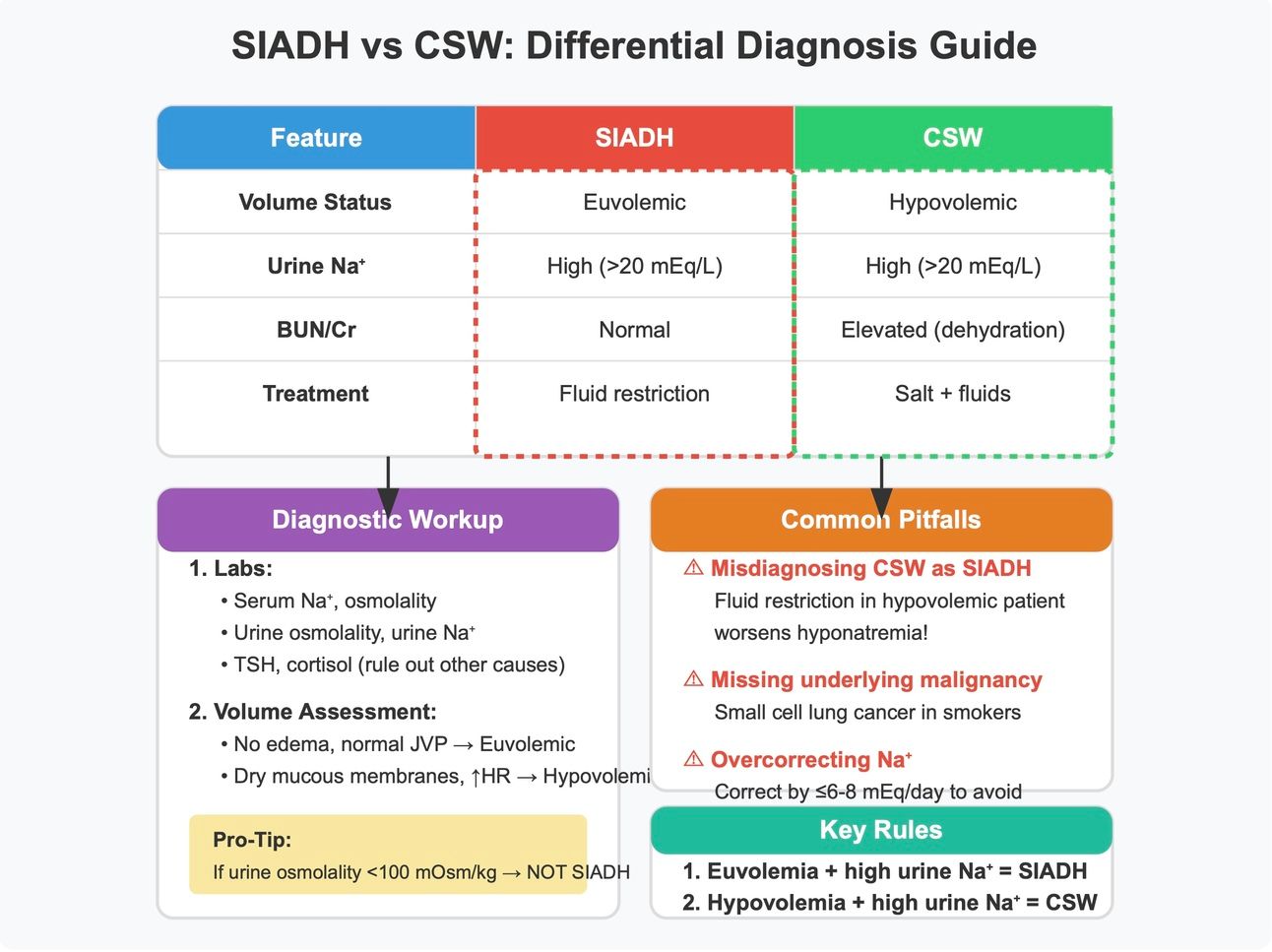
Visual Cheat Charts 📈
Stay Hungry, Stay Curious!
Your Brother in This Struggle
Dr. Shoaib Ahmad
